| Index | Next |
Case 9 Clinical History
Case 10 Clinical History Diagnosis Discussion
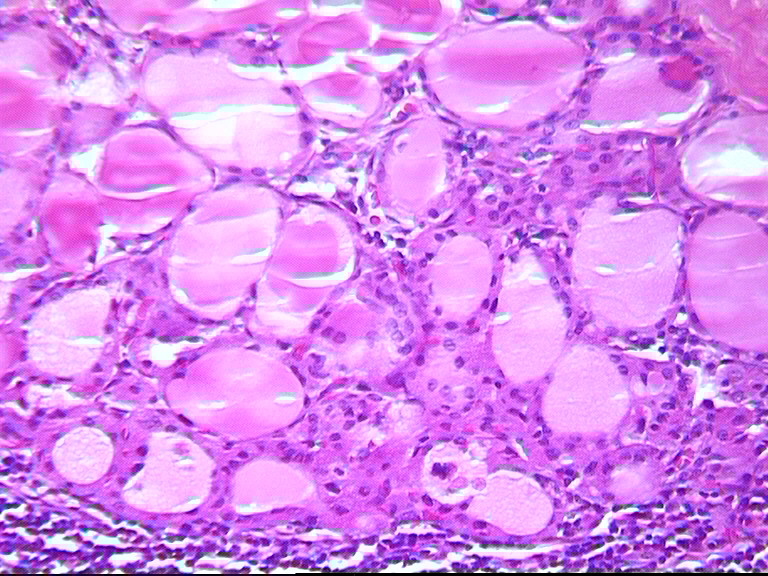
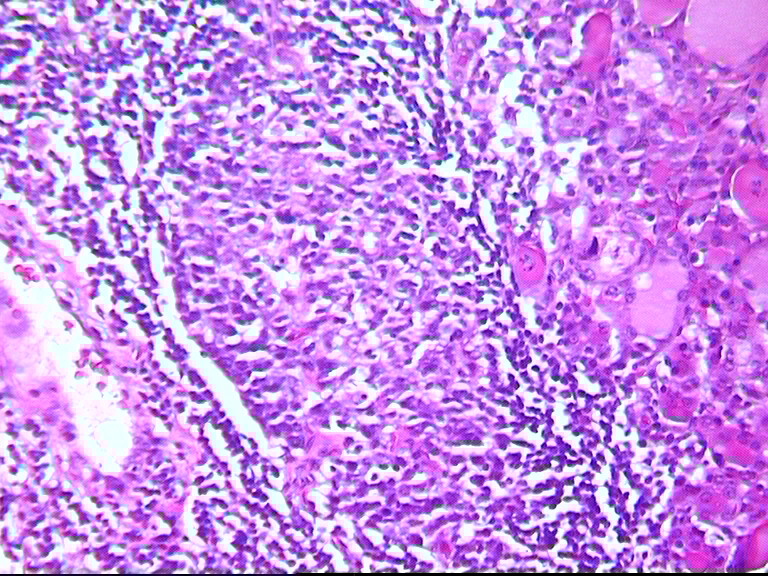
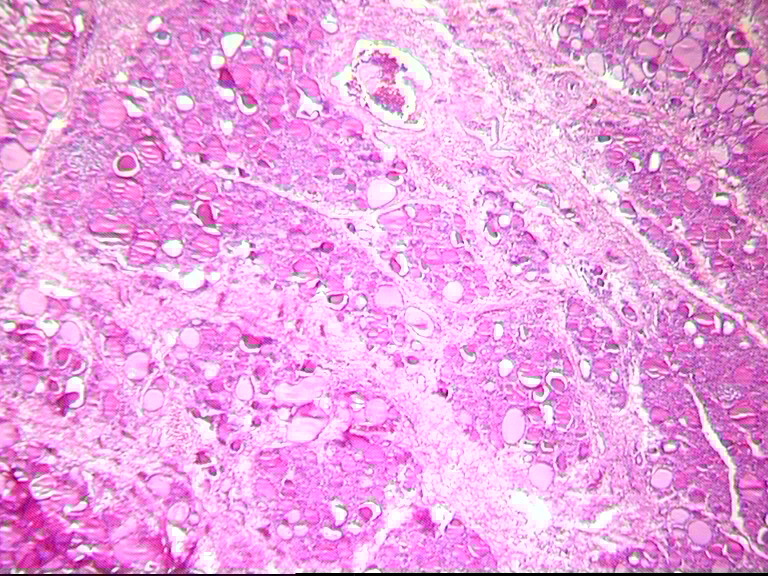
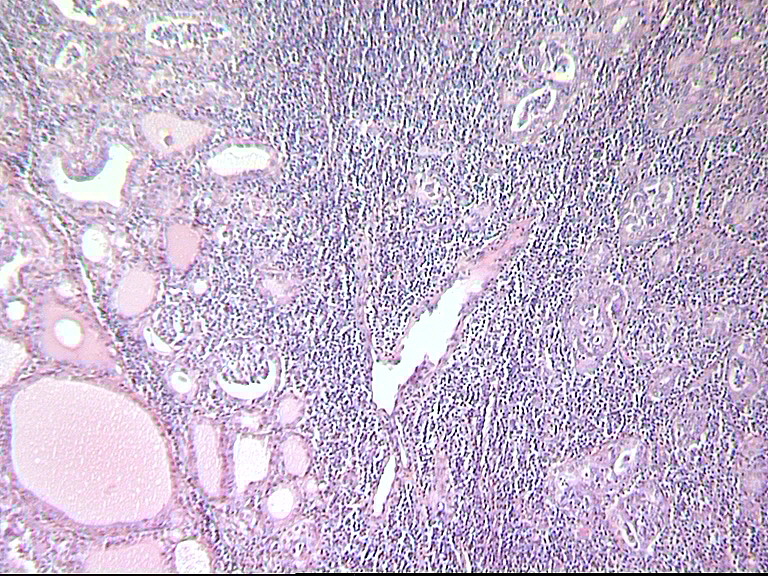
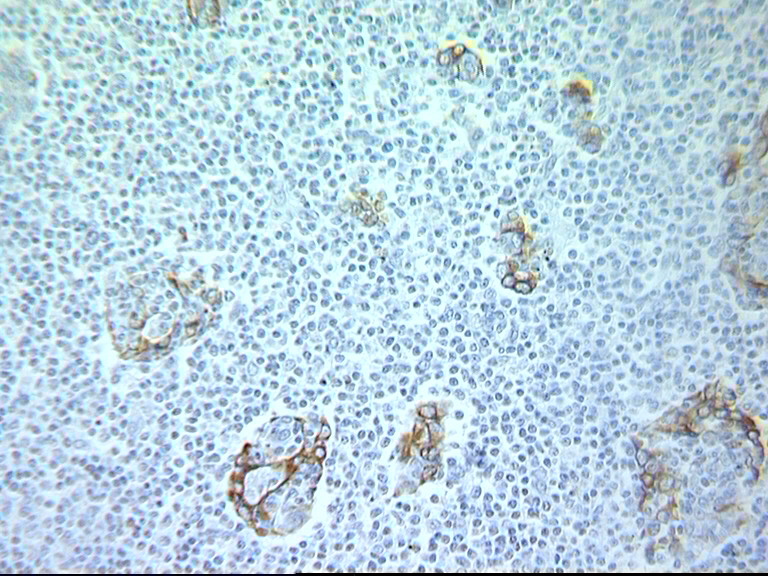
Primary lymphomas of the thyroid (PTL) occur predominantly in middle aged and older women in a setting of Hashimoto’s disease. They represent 5% of thyroid cancers and 2,5 to 7% of extranodal lymphomas PTL are presently believed to belong to the group of lymphomas deriving from the mucosa-associated lymphoid tissue (MALT),and called accordingly MALT-lymphomas. PTL are essentially B-cell lymphomas containing moncytoid B-cells and centrocyte-like cells. They may show an important plasmacytoid differentiation with numerous Dutcher bodies. They may present normal reactive follicles or follicles colonized by lymphomatous cells. The identification of these colonised follicles can be made by the Bcl2 immunohistochemical staining which is positive in normal germinal centers and in follicles of follicular center-cell lymphomas but negative in colonized follicles. PTL are devided in 3 groups : 1) MZBL : The low grade lymphoma of MALT called marginal zone B-cell lymphoma, made essentially of small lymphoid cells of the centrocytic-like or marginal type. 2) DLBCLA : The high grade lymphoma of MALT made mostly of large cells of the immunoblastic or/and centroblastic type ; they are labelled as diffuse large B-cell lymphomas. 3) Mixed MZBL and DLBCL : A high grade lymphoma derived from a low grade lymphoma with zones of passage from the one form to the other. High grade lymphomas form the majority ( 60% ) but despite this fact, the prognosis of high grade lymphomas depends more on the stage than on the type. Indeed stage IE high grade lymphomas are faring quite well when compared to nodal lymphomas of a similar type. Other factors seem to play a role in the prognosis such as necrosis, apoptosis, number of mitoses, and presence of vascular invasion. As mentionned previously, stigmata of Hashimoto’s thyroiditis can be found in the majority of cases even in the high grade PTL but they are better evidenced in low grade lymphomas. Light- chain restriction is present in PTL but cannot always be demonstrated , as for instance in fixed material.
Fonseca A, Sambade C Deringer GA, Thompson LDR, Frommelt RA, Bijwaard KE et al.
|


Copyright 2002, The Author(s) and/or The Publisher(s)
| Organisation: FORPATH asbl |
Coordination: Dr Bernard Van den Heule |
Host: Labo CMP |