| <<< Previous | Index | Next >>> |
Case 1
Clinical and haematological data.
69-yr-old lady. A diagnosis of lymphoma, diffuse large B-cell (REAL/WHO) was made in a cervical LN. No other
adenopathy, no hepatosplenomegaly.
PB count and smear within normal range.
BM aspirate : overall normal BM cellularity. One/12 smears characterized by a lymphocytic
infiltrate, exhibiting small lymphocytes with mature chromatin.
Bilateral BM biopsy performed .
Both biopsies show an overall cellularity within normal range, although somewhat
heterogeneous. Three cell lines present with maturation. Several lymphoid aggregates or "nodules", are
present. They are not paratrabecular in position, well circumscribed, and composed of small-sized lymphocytes exhibiting a very slight
pleomorphism.
At IHC examination, mixed B- and T- cell population, both in the aggregates and
interstitial.
A few polyclonal plasma cells.
Diagnosis and interpretation. BM lymphocytosis, interstitial and focal, most consistent with a reactive
process; absence of involvement by a large B-cell lymphoma.
Comments
The interpretation of lymphoid nodules is often a difficult task, although some guidelines exist
(see Table 4). No absolute criteria! The application of flow-cytometry
and/ or molecular biology on BM and/or PB is certainly of help in difficult situations.
The lymphoid aggregates of our patient present many features in favour of a reactive
process: "non-paratrabecular" localisation, no frank cytological atypia and mixture of B - and T-cells at IHC
examination. Note that neoplastic nodules of B-cell lymphomas are most commonly composed of an homogeneous B-cell population but exceptions do
exist.
Benign lymphoid aggregates are relatively common findings in BM biopsy. The incidence appears to increase with age and is higher in females than males. The aggregates may occur in patients with a wide range of
disorders. Usually large aggregates may occur in the BM of patients with diseases related to the immune system such as autoimmune
disease, HIV infection, thymoma, old age... In the case presented here, an important point is to exclude BM involvement by a low-grade component of the large B-cell lymphoma diagnosed in LN. According to Brunning and Mc Kenna (1994), histological discordance between the LN and BM is observed in 15 to 40 % of the cases.
In our patient, flow cytometry applied on the BM lymphocytes was in favour of a reactive
process: predominantly small T-cell population and absence of B-cell
monoclonality.
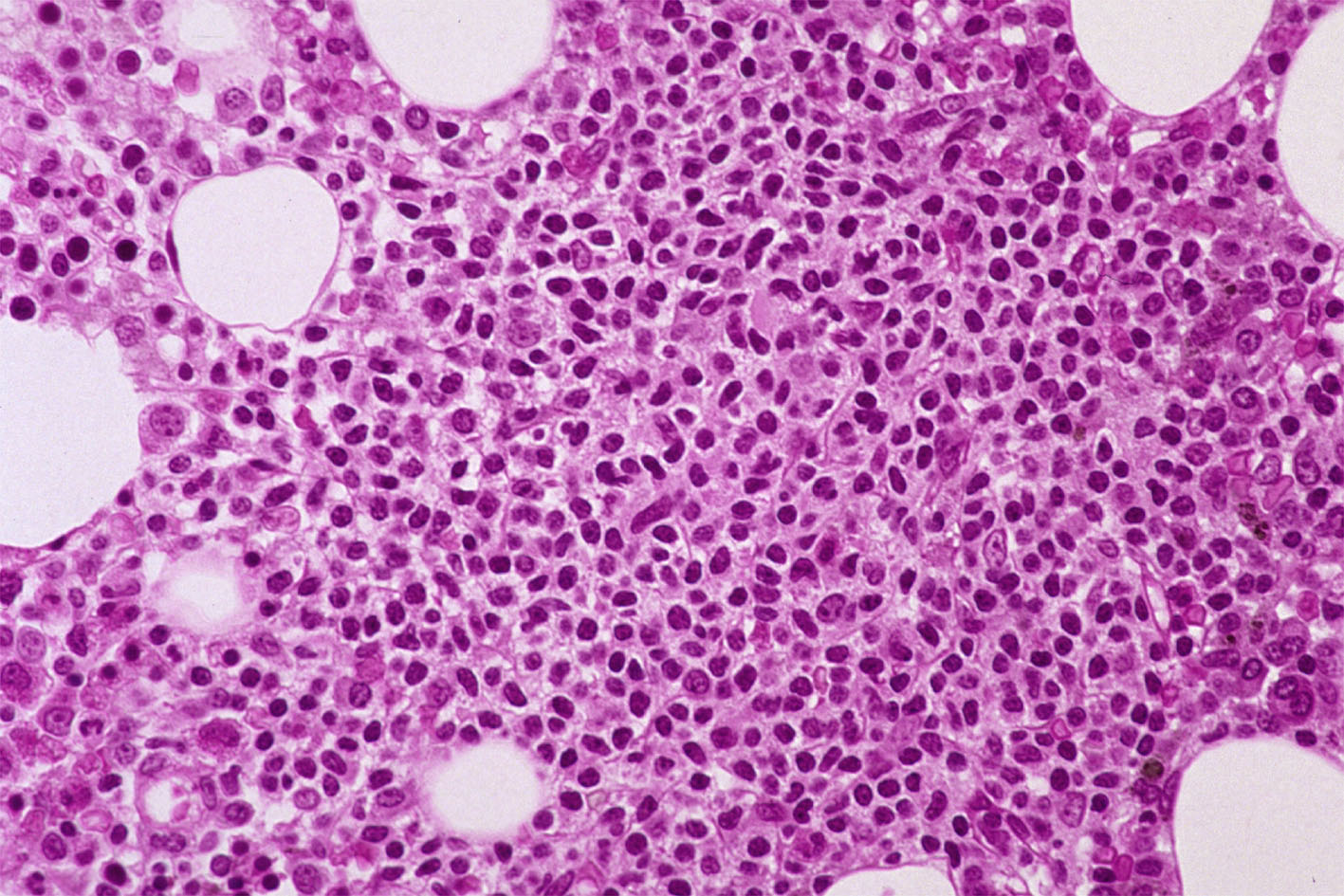
Case 1. BM lymphocytosis, reactive process.
| <<< Previous | Index | Next >>> |
Copyright 2001, The Author(s) and/or The Publisher(s)
| Organisation: FORPATH asbl |
Coordination: Dr Bernard Van den Heule |
Host: Labo CMP |