| <<< Previous | Index | Next >>> |
Case 4
Clinical and haematological data.
73-yr-old man. Suffers from fatigue. Presented with splenomegaly and pancytopenia. No adenopathy, no hepatomegaly.
Hb 72 g/l, L 1,6 G/l, T 109 G/l
No atypical cells described on PB smear.
BM examination
Dry tap at BM aspiration
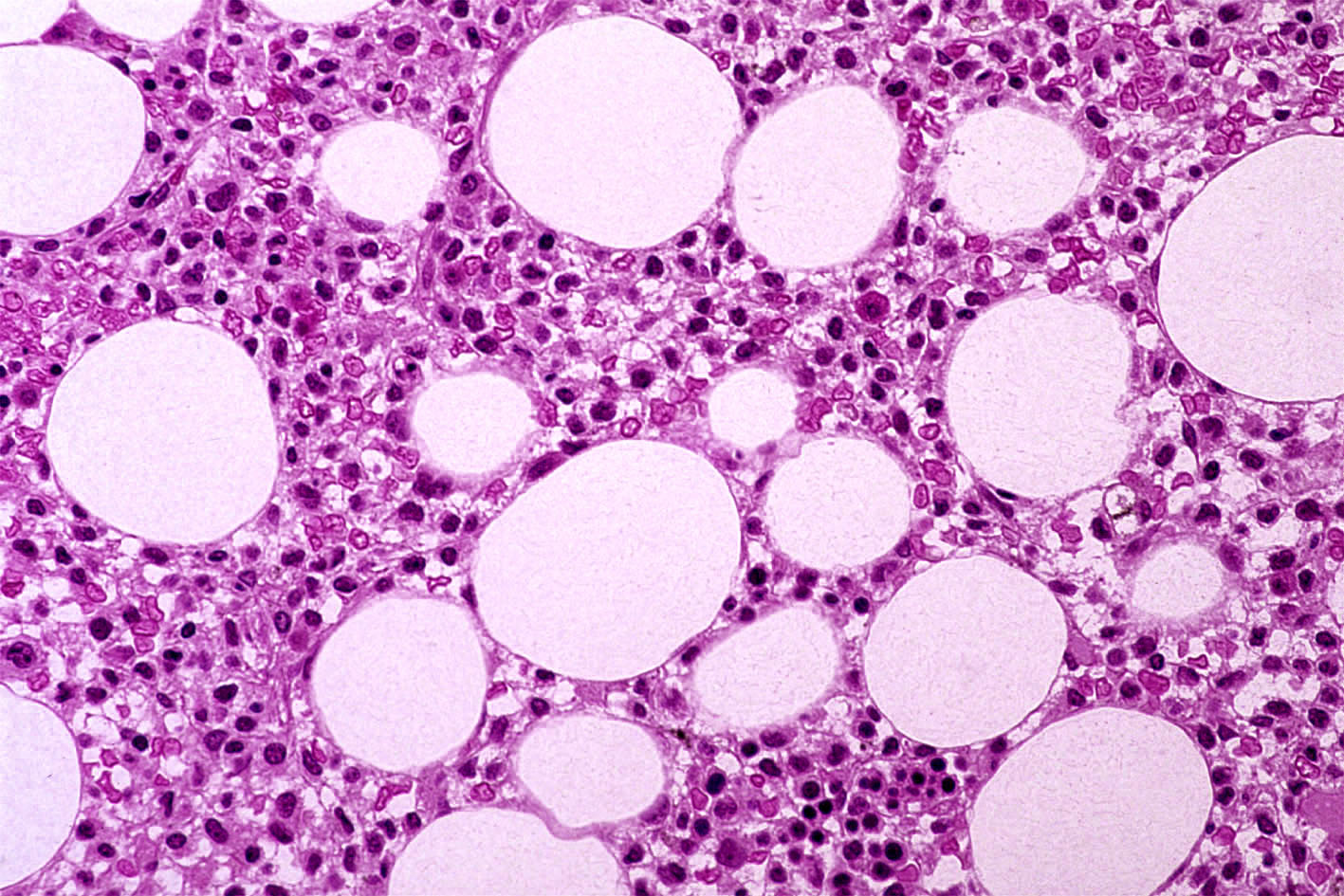
BM trephine reveals an interstitial and loose infiltration by small to medium sized cells with bean-shaped or indented nuclei, surrounded by a clear zone. Decreased haemopoiesis. Moderate and diffuse increase in reticulin.
IHC: the atypical cells are positive for B-cell markers with a strong positivity for DBA44. Tumour cells negative for CD 3, CD 34 and MPO.
Interpretation and diagnosis: Morphology and IHC results typical of Hairy Cell Disease (HCD) with "hypoplastic" BM.
Comments
HCD is a disease of the adult age group (mean age 50 yrs; range 24-80 yrs) with a M:F ratio of 5:1. Splenomegaly is present in 90 % and hepatomegaly in 50 % of the cases. Lymphadenoapthy is uncommon.
The PB counts always reveal variable degrees of cytopenia, 75 % of the patients presenting with pancytopenia. Monocytopenia is frequent and has been implicated in the pathogenesis of the infections which characteristically accompany the disease. The proportion of hairy cells on the PB varies from case to case and may be rare and difficult to find (only 25 % of the patients have more than 50 % hairy cells in the differential count).
A diagnosis of HCD, suspected on the basis of clinical and haematological features needs a confirmation by either cytochemical*, histological or immunological methods.
BM is always involved. BM aspirate is usually unsuccessful due to increase in reticulin fibres.
BM histology represents a reliable diagnostic tool and the histopathologist can make the diagnosis with confidence. BM trephine and IHC are necessary for the differential diagnosis with other lymphoproliferative disorders. BM biopsy shows a diffuse infiltration by hairy cells in most cases. Fibrosis is typical. Hairy cells infiltrate the BM in a very characteristic loose fashion with a well-defined rim of cytoplasm which leaves a clear zone around the cells. These appearances facilitate the differential diagnosis from other lymphoproliferative disorders. In a minority of cases, patchy infiltration may be seen, more frequently in early stages of the disease. Rare cases of HCD are characterized by an interstitial infiltration together with a hypoplastic BM. Such cases should not be confused with an aplastic anaemia. Classically, hairy cells are small to medium sized, with oval or "bean"-shaped or indented nuclei. Nucleoli and mitotic activity are inconspicuous. The "hairy" features of cytoplasms are not visible on tissue sections
IHC. Tumour cells are positive for B - cell markers (L26/CD20, DBB42). The positivity for DBA44 is highly characteristic of HCD, although not entirely specific. According to the literature and our experience,
IHC - especially DBA44 immunostaining - is mandatory for the detection of subtle interstitial infiltration or residual disease after treatment (example shown: slide 4 b)
*Hairy cells also have tartrate resistant acid phosphatase (TRAP) activity. This cannot be applied routinely on tissue sections but can be performed on imprints from the biopsy.
Case 4. Hairy Cell Disease.
| <<< Previous | Index | Next >>> |
Copyright 2001, The Author(s) and/or The Publisher(s)
| Organisation: FORPATH asbl |
Coordination: Dr Bernard Van den Heule |
Host: Labo CMP |