| <<< Previous | Index | Next >>> |
Case 9
Clinical and haematological data
33-yr-old woman, HIV+. Presented with fever and jaundice.
History of gastro-enteritis 2 weeks ago.
Hepatosplenomegaly. No peripheral adenopathy. Retroperitoneal adenopathy on CT scan.
Therapy: Ciproxine, Fenoxypen
Lymphoma and/or opportunistic infection suspected.
Hb 82g/l, L 1.4 G/l, T 148.
PB smear : macrocytic anaemia, neutropenia, lymphopenia.
BM aspirate: normocellular BM with dysmyelopoiesis of the 3 cell lines, strong plasmacytosis, 5% lymphocytes, absence of opportunistic microorganisms, absence of lymphoma.
BM biopsy (unilateral): increased cellularity, three cell lines present, dyserythropoiesis, shift to left of the granulocytic cell line, increased number of megakaryocytes, dysmegakaryopoiesis (small forms, hypolobulated nuclei, apoptotic nuclei), increased number of plasma cells, a few epithelioid and histiocytic cells, very rare atypical large nucleolated cells observed on some levels of section, special staining for microorganisms negative.
IHC: polyclonal plasmacytosis, slight lymphocytosis with a mixture of B- and T- cells; no atypical cell positive for CD30.
Interpretation and diagnosis
Non specific reactive BM in the context of an HIV infection.
Rare atypical - but non-diagnostic - large nucleolated cells (Hodgkin's cells?)
Because of the suspicion of lymphoma, liver and retroperitoneal adenopathy biopsies were performed. Both biopsies disclosed Hodgkin's disease, mixed cell type with granulomatous reaction.
Comments
Peripheral blood (PB) cytopenia is one of the major indications for BM examination in HIV-positive patients and t
his case illustrates the complexity of the BM analyse in the context of a HIV infection. The BM trephine presented here exhibits a constellation of findings, which are characteristic - although not specific - of HIV infection: hypercellularity with increased number of megakaryocytes, plasmacytosis, fibrosis and dysmyelopoiesis (especially dysmegacaryopoeisis). Gelatinous transformation of the stroma, opportunistic infections and lymphoma may also be observed in advanced disease
Our case is an example of dysmyelopoiesis or myelodysplastic features associated with a reactive process. Hyperplasia of the megakaryocytic cell line together with dysmegakaryopoiesis represent the histological hallmark of the ineffective thrombocytopoiesis in HIV infection. In this context, the term "dysmyelopoiesis" is used in a descriptive sense, referring to "maturation abnormalities" of the haematopoietic cell lines and does not imply a "premalignant state". The pathogenesis of the haematological abnormalities in HIV infection appears to be multifactorial: coexisting infections, neoplasm, drugs, antibodies against PB elements, circulating immune complexes, hypersplenism and HIV itself are potential candidates. Both in vitro and in vivo studies have shown that megakaryocytes are susceptible to HIV infection.
The diagnostic of Hodgkin's disease (HD) in BM trephine may be a challenge for the histopathologist. Because of the heterogeneity of the infiltration, diagnostic foci may be overlooked. HD in HIV-infected patients has been reported mainly in Europe. An unusually aggressive tumour behaviour has been reported, including higher frequency of unfavourable histologic subtypes, advanced stages, extranodal involvement and poorer therapeutic outcome, as compared with the behaviour of HD outside of the HIV setting.
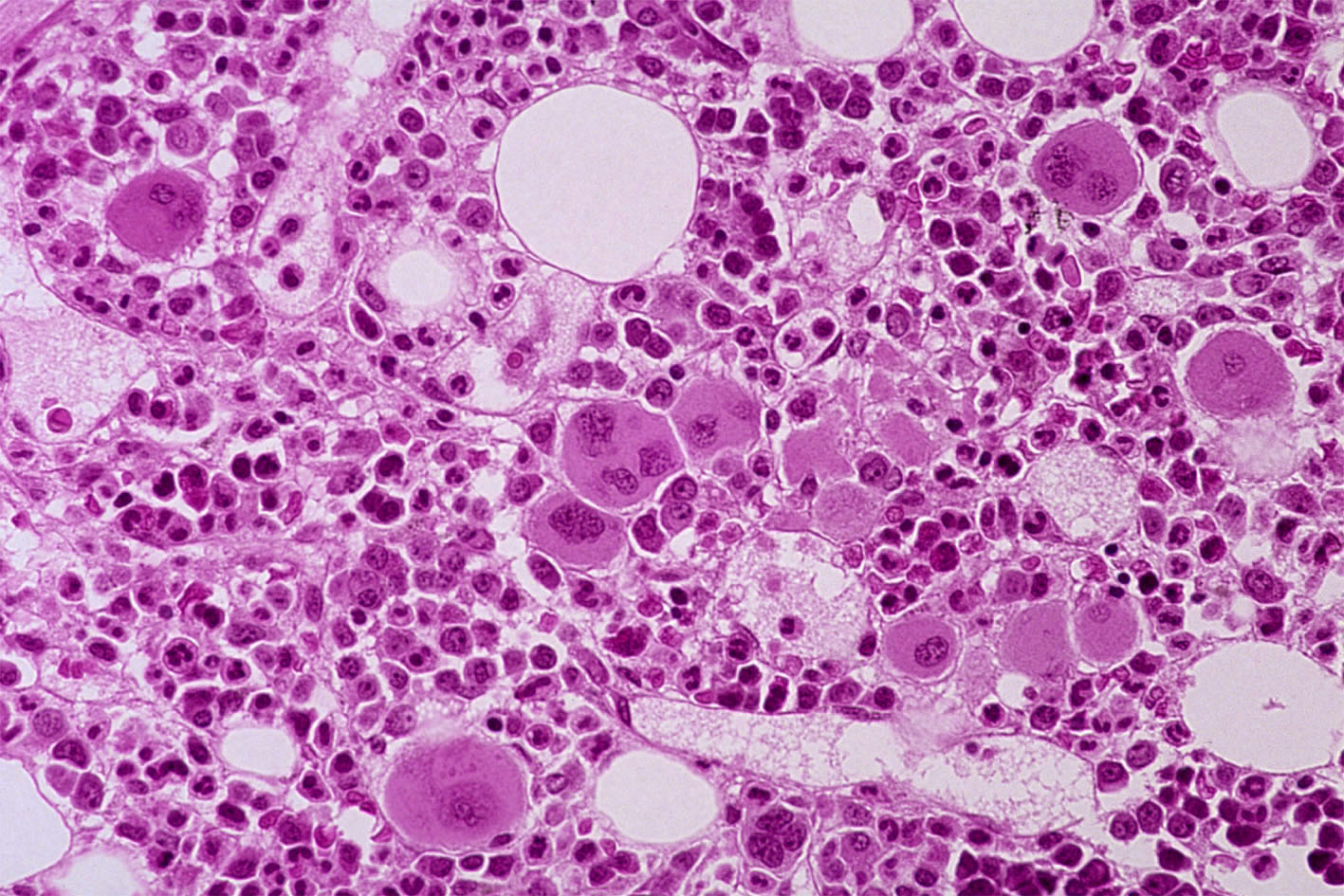
Case 9. Reactive BM in the context of an HIV infection.
| <<< Previous | Index | Next >>> |
Copyright 2001, The Author(s) and/or The Publisher(s)
| Organisation: FORPATH asbl |
Coordination: Dr Bernard Van den Heule |
Host: Labo CMP |